The detox went fine. That was the strange part. The body cleared, the bloods came back steadier, the shaking stopped, and for a week or two there was a kind of quiet that everyone mistook for recovery. Then the quiet filled up with something else. The anxiety the drinking had been holding at bay came back without an anaesthetic. The flashbacks returned. And within a month, sometimes within a fortnight, the person was back where they started, and the family was left wondering what they had done wrong.
They had not done anything wrong. They had treated half the problem.
This article explains what dual diagnosis treatment actually is, who it is genuinely for, and what integrated residential care looks like when it is done properly – not as a concept, but as a lived daily structure that gives two tangled conditions room to be addressed at the same time.
Reading time: 9 minutes
Key Points
- Dual diagnosis is not two separate illnesses sharing a body – it is one interlocking pattern where a mental health condition and a substance use disorder feed each other, and treating only one reliably fails.
- Residential treatment creates the distance and daily structure that outpatient care cannot provide when the pattern is entrenched – and that distance is often the difference between a stay that holds and another failed attempt.
- Genuine integrated care means one team, meeting daily, coordinating medical, psychiatric, and therapeutic work around the same person – not two appointments running past each other.
- You do not need a formal diagnosis before asking for help. Assessment is part of what the first days of a serious programme are for.
Table of Contents
- What dual diagnosis actually means
- Dual diagnosis or co-occurring – is there a difference?
- Does integrated treatment have to be residential to work?
- Who residential dual diagnosis treatment is actually for
- How to tell it is dual diagnosis and not just addiction
- Do you need a formal diagnosis before starting?
- What integrated treatment looks like in practice
- The therapies you are most likely to meet
- Is psychiatric medication part of dual diagnosis treatment?
- When there is trauma or PTSD underneath
- A day inside a residential programme
- How long it takes, and what the minimum really is
- Residential, inpatient, PHP, IOP – what the acronyms mean
- What family does, and the thing it has to stop doing
- Questions worth asking before you choose a centre
- What it costs, and what the price is buying
- After residential – the part that decides whether it lasts
- Where Holina Village fits
What dual diagnosis actually means, defined by what it is not
It is not two separate illnesses that happen to share a body. That is the assumption that breaks so much treatment.
It is one interlocking pattern. The mental health condition raises the pull toward a substance that quiets it. The substance, over time, deepens the mental health condition. The National Institute of Mental Health describes how substance use disorders and mental disorders share genetic and environmental risk factors and act on overlapping circuits in the brain – which is the clinical version of what families already sense: that you cannot pull one thread without the other moving. You can read their summary of the overlap in the NIMH overview of substance use and mental health.
So the modern standard is integrated care under one roof, with one team. Treat the addiction alone and the unaddressed mind reignites it. Treat the mind alone and the substance keeps sabotaging the work. The relapse data on split, uncoordinated care is not subtle.
“Dual diagnosis” or “co-occurring” – is there a difference?
People ask this constantly, usually worried they have stumbled into two different things.
They have not. Clinically, dual diagnosis and co-occurring disorders describe the same situation: a substance use disorder and a mental health condition present at the same time. The shift toward “co-occurring treatment” in recent years was partly a move to soften the weight of the word “diagnosis,” which carries a psychiatric heaviness that keeps some people from picking up the phone at all.
The label changed. The work did not. Whether your search history reads “dual diagnosis rehab” or “co-occurring treatment,” you are looking for the same thing.
Does integrated treatment have to be residential to work?
Outpatient therapy has genuine value. For many people, a weekly session with a good psychologist is exactly enough, and we would never pretend otherwise.
It reaches its limit when the two conditions are amplifying each other in real time. An hour on a Tuesday cannot compete with a home full of triggers, easy access to the substance, the same social circle, the same late-night spiral, and a nervous system that has learned only one way to settle itself. When the pattern is that entrenched, the most useful thing you can give someone is distance. A contained space where the old cues are simply not present, where the day is held by other people, where round-the-clock support means a hard hour at 2am is not faced alone.
That is the case for a residential setting, and for complex dual diagnosis it is often the difference between a stay that holds and another failed attempt. At Holina Village, the point of living somewhere green and quiet is not luxury. It is that the work has room to happen – something you can read more about in the full residential programme overview.
Who residential dual diagnosis treatment is actually for

Not everyone needs it. So it is worth being specific about who does.
The person whose moods swing hard, who lives with severe anxiety or panic or clinical depression, and who has been reaching for alcohol, drugs, or sedatives as a form of self-medication. The person who has tried treatment before and watched it unravel within weeks of going home, because they went home before they had built any new way of regulating themselves. The younger adult, or the older one, whose daily functioning has fallen apart, whose relationships keep breaking, who has slipped into a loop of self-harm or isolation that nobody around them can interrupt.
If you recognise someone in that description, residential dual diagnosis treatment is built for exactly that profile. The intensity is the point. So is the time away.
How to tell it is dual diagnosis and not “just” addiction
There is a tell, and once you see it you cannot unsee it.
The substance is being used as a solution, not a pleasure. It is taken to switch off intrusive thoughts, to dull a flashback, to fill a flat emptiness, to make a body that runs too hot or too numb feel briefly liveable. The second tell is what happens in sobriety. If the anxiety, the dread, the emotional intensity are still there after the substance has cleared – after a first detox – then the mind was never the passenger. It was driving.
The third tell is the crash. As the substance wears off, the mental state does not return to baseline. It drops below it. The screening literature stresses that this overlap makes early diagnosis genuinely difficult, which is why assessment continues over time rather than being settled on day one.
None of this makes the person weak-willed or lazy. It makes them someone carrying two loads at once, on a nervous system that has been pushed past where it can cope alone.
Do you need a formal diagnosis before starting?
No. This is the question that stops people, and the answer is no.
Most people arrive without a clear picture of what is wrong. They come with a partial diagnosis, an old one, a wrong one, or none at all. A serious centre does not require you to have it sorted in advance. The first days of a good dual diagnosis rehab are an assessment period – a proper clinical evaluation that draws on a psychiatrist, therapists, and clinical staff, and that keeps refining itself as the substance leaves the system and the underlying picture becomes legible.
You do not need to understand your own problem before you ask for help with it. Understanding it is part of what the help is for.
Not sure where to begin?
If you are trying to make sense of what you or someone you love is carrying, an honest conversation with the Holina team is a good place to start. No pressure, no obligation.
Reach the Holina Village team for a confidential conversation
What integrated treatment looks like in practice, not just on paper

There is a version of “treatment for both” that is really just two programmes running past each other. A private psychiatrist on a Wednesday. A separate support group on a Friday. Neither one talking to the other. The psychiatrist does not know what came up in group. The group does not know the medication changed. The person becomes the only point of contact between two teams who never meet, which is a lot to ask of someone in crisis.
Real integrated care closes that gap. The medical, psychiatric, and therapeutic staff meet about the same person, daily or weekly, and coordinate. The trauma work and the relapse-prevention work are built together, so that a hard therapy session does not blow up the recovery plan and the recovery plan does not stall the deeper work.
That coordination is the whole difference between co-occurring treatment and two appointments in a row. Done properly, this is also where the clinical team earns its keep, because the work happens in the conversations between sessions as much as in the sessions themselves.
The therapies you are most likely to meet
No single method carries a dual diagnosis. A few, used together, do most of the load.
What CBT and DBT each do
Cognitive behavioural therapy goes after the thought patterns that light the fuse: the all-or-nothing thinking, the catastrophising that floods someone with anxiety and then hands them a reason to use. It is practical and it is teachable. Dialectical behaviour therapy works further down, on the raw machinery, when there is impulsivity, self-harm, or emotional storms that arrive faster than thought. It teaches concrete skills. Distress tolerance for the worst hour. Mindfulness for the noise. A way through a crisis that does not end in a drink or a blade.
ACT and Motivational Interviewing
Acceptance and commitment therapy stops fighting the existence of pain and starts asking a harder question: what is this life actually for. It works through a person’s own values, building reasons to stay clean that belong to them rather than to anyone else. Motivational interviewing meets the part of someone that does not want to change at all, without arguing with it, lowering the resistance and the shame that so often guard the door. The behavioural and medical evidence behind these approaches is summarised in NIDA’s research overview of addiction treatment and recovery.
Is psychiatric medication part of dual diagnosis treatment?
For many people the word “medication” sets off an alarm. They came to get off substances. Now someone is suggesting a prescription.
The fear is understandable and the distinction matters. A non-addictive, carefully monitored medication is a different thing entirely. An antidepressant, a mood stabiliser, a non-addictive sleep aid. Sometimes the psychiatrist’s job is simply to make the inside of someone’s head quiet enough that they can sit in a therapy room and actually hear what is being said. Without that floor of stability, the psychological work has nothing to stand on.
Medication does not replace the therapy in good dual diagnosis treatment. It makes the therapy possible.
When there is trauma or PTSD underneath
This is the combination that catches the most people out, and it has its own rules.
A traumatised nervous system lives at one of two poles. Hyperarousal, where everything is too loud and too close. Or dissociation, where the person is barely present at all. A substance offers a temporary off switch for both. That is why trauma and substance use travel together so often – a link laid out plainly by the National Center for PTSD in its explanation of the connection between substance use and PTSD.
The mistake is rushing toward the traumatic memories. You do not open those in the first days of withdrawal. That floods an already overwhelmed system and tends to send people straight back to the substance. The order is the opposite. First the safety. First the soothing kit, the physical anchors, the breath, the felt sense of being somewhere contained. Only once that ground is steady does the deeper processing begin, and even then, slowly.
A day inside a residential programme
People imagine something institutional. A locked ward, a corridor, a sense of being put away. The reality of a good residential day is closer to a structured rhythm than a confinement, and the structure itself is part of the medicine.
The morning starts on time, with a real breakfast, because a body that has been running on substances needs feeding back into shape. A short group practice or a few minutes of mindfulness to bring the anxiety down and set an intention. Late morning is the clinical heart of the day: psycho-educational groups, processing groups, one-to-one sessions with a therapist. The afternoon turns toward the body and the natural world. Time on the farm, hands in the soil, the animals, gentle movement, an art session – the kind of activity that lets the brain produce its own dopamine instead of buying it.
Evening is communal. A shared meal, a support meeting, then quiet. Journalling. Sleep at a fixed hour, because repairing the sleep cycle repairs more than people expect. The farm setting feels nothing like a clinical facility, and that is deliberate. For some, the time outside becomes its own thread of the work, which is part of why the adventure and outdoor activities at Holina sit inside the programme rather than beside it.
How long it takes, and what the minimum really is
There are no weekend cures. Anyone selling one is selling something.
Dual diagnosis takes longer than uncomplicated addiction, and there is a biological reason. The dopamine system and the circuits the substance hijacked need weeks to start recalibrating before any durable psychological change can take hold. A four-week stay lets the nervous system begin to settle. It is around the eight-to-twelve-week mark that new patterns start to actually hold rather than just appear.
Research from the National Institute on Drug Abuse is explicit that programmes shorter than ninety days show limited effectiveness and that longer durations are tied to better long-term outcomes. Good programmes tend to run between 60 and 90 days for this reason, and the clinical reasoning behind that is set out clearly in their principles of effective drug addiction treatment.
Residential, inpatient, PHP, IOP – what the acronyms mean
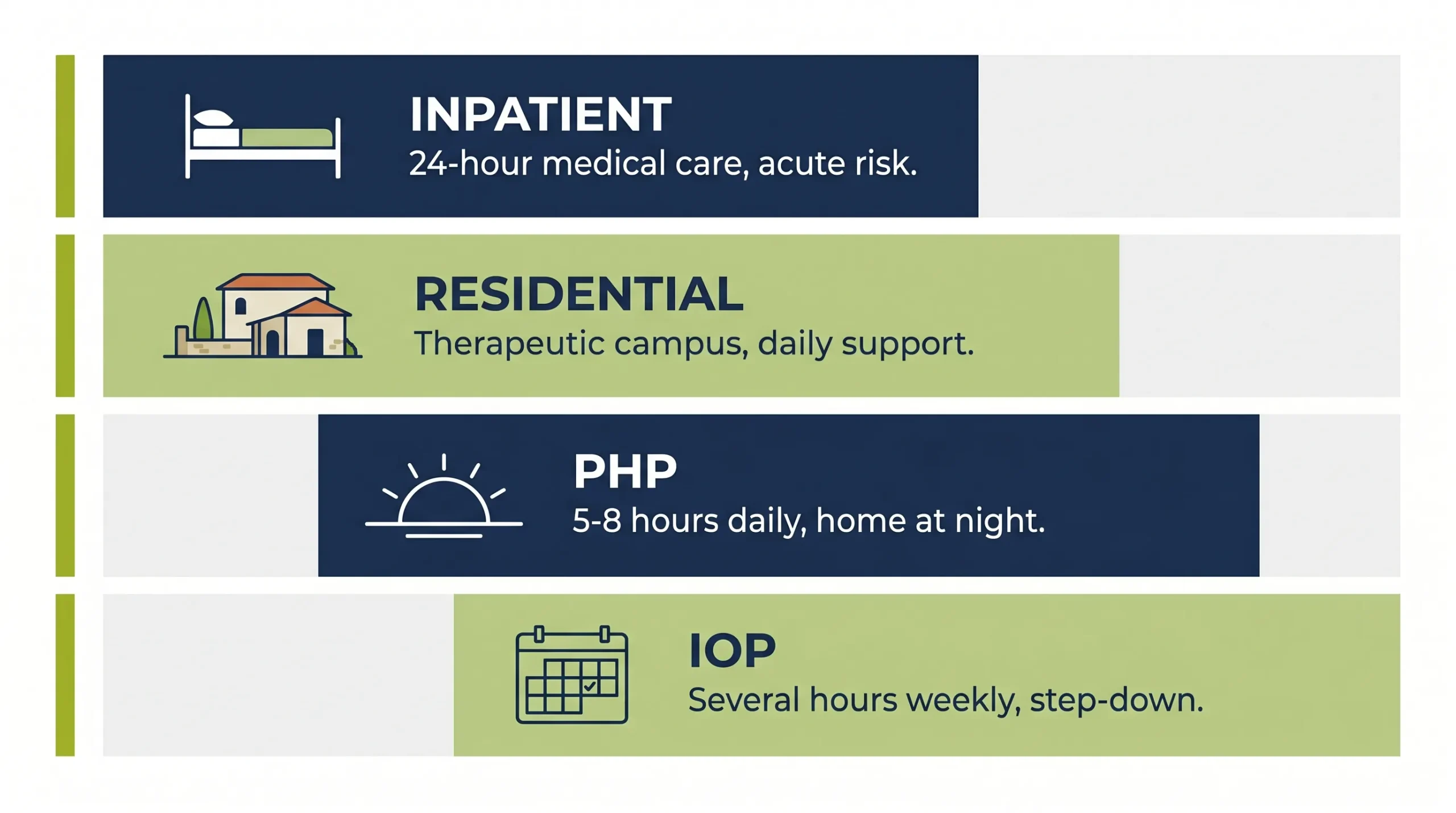
Families researching centres abroad hit a wall of English-language jargon at exactly the moment they have least patience for it. Here is the plain version.
| Level of care | What it is | Best suited for |
|---|---|---|
| Inpatient (hospital) | Full hospital admission with 24/7 medical and nursing cover | Acute psychosis, immediate medical risk, complex medical detox from alcohol or benzodiazepines |
| Residential | Living on a therapeutic campus with a multidisciplinary team and psychiatrist on hand, warm rather than clinical | Complex dual diagnosis needing distance from triggers and daily support |
| PHP | Around 5-8 hours of treatment a day, returning home or to supervised housing at night | People stable enough to sleep off-site but needing intensive daily care |
| IOP | A few hours, several times a week, of individual and group work | A step-down phase, re-entry, returning to work or study |
A residential programme delivering integrated co-occurring treatment usually sits between the hospital and the day programmes, which is where most complex cases belong.
What family does, and the thing it has to stop doing
If you are the parent, the partner, the sibling reading this at an hour you should be asleep, this section is for you.
The hardest thing to hear is about enabling. When a family keeps clearing the consequences, paying the debts, smoothing the fallout, making the next day survivable, they are loving someone in a way that quietly removes every reason to change. The consequences are part of what eventually moves a person toward help, and softening all of them can postpone that for years.
This is not a call to abandon anyone. It is the opposite. Family therapy teaches the difference between a boundary and a punishment, between support and rescue, and it does it without blame, because most families have been improvising in the dark. Holding a steady line while keeping the door open is a skill, and it can be learned. Done well, this is the heart of dual diagnosis treatment that reaches past the individual.
Questions worth asking before you choose a centre
A scared family is an easy family to reassure with words. The questions below are designed to get past the words.
Ask whether there is a licensed psychiatrist on the core team, or whether one is only called in during a crisis. The difference tells you how seriously they take the mental health half. Ask what proportion of the therapists hold full clinical licences – real psychologists and accredited mental health social workers, rather than peer mentors alone. Ask how they prevent a person being destabilised when trauma surfaces, because if they cannot answer that clearly, they probably destabilise people.
And ask what the aftercare looks like, in concrete terms, for the day the person walks out. A residential stay without a re-entry plan is a held breath, not a recovery.
What it costs, and what the price is buying
The number is real and it is worth understanding honestly. The cost of residential care is not mostly accommodation and meals. It is the clinical density: the hours of senior clinicians, the psychiatrist, the trauma specialists, the complementary therapies, and the low ratio of residents to staff that makes individual attention possible. A high staff ratio is the single thing most worth checking.
At Holina, the tiers are all-inclusive, covering clinical and group sessions, meals, farm and adventure activities, and airport transfers, with personal spending money the only extra.
| Room tier | From (per month) | What is included |
|---|---|---|
| Shared Room | €7,950 | Full clinical programme, meals, groups, farm and adventure activities, transfers |
| Single Room, Shared Bathroom | €10,950 | As above, with private sleeping space |
| Single Room, Private Bathroom | €12,950 | As above, with full private facilities |
The clinical content of residential dual diagnosis treatment is identical across the tiers. What changes is privacy, not care.
After residential – the part that decides whether it lasts

The campus is protected. The world is not. The weeks after discharge are where most relapses happen, and they are where the planning has to be most exact.
A genuine relapse-prevention plan is not a pep talk. It is a set of rehearsed responses for the specific moments that will come: the sudden emotional storm, the chance meeting with someone from the old life, the ordinary Tuesday that turns dangerous. It includes a real handover to local outpatient care, regular psychotherapy and psychiatric follow-up near home, so the support does not fall off a cliff at the airport.
It depends on keeping the rhythms that were rebuilt inside: the sleep, the movement, the time outside, the food that helps the brain heal, and the willingness to reach for help at the first slip rather than the tenth. Good clinical research frames relapse as part of managing a chronic condition rather than a verdict – which changes how a family responds when it happens.
Where Holina Village fits
Everything above describes a problem with a particular shape: two conditions tangled together, needing distance, time, and a team that talks to itself. Holina Village was built around that shape.
It is a residential campus in Achnas, Cyprus, close enough to Israel and to Europe that reaching it is simple, far enough that the old triggers do not follow. Green, quiet, with orchards and animals and open sky – somewhere a tense nervous system can finally stand down. The therapeutic community gives people the relational substrate that so much of this work depends on: shared responsibility, shared meals, the slow rebuilding of an ordinary functional life among others doing the same. The programme runs evidence-based therapy – CBT, DBT and ACT – alongside trauma-sensitive work, steady psychiatric and medical support, and the body-and-mind practices that hold it all together.
Frequently Asked Questions
Dual diagnosis is one problem with two faces, and the treatment that works addresses both at the same time, in the same place, with a team that is in constant contact with itself. Residential care provides what outpatient care cannot when the pattern is entrenched: distance, structure, time, and a daily environment where the old cues lose their grip. The therapies – CBT, DBT, ACT, trauma-informed work, and the steadying routines of a farm setting – are built to work together, not alongside each other.
If any of this feels like the situation you or someone you love is in, the Holina Village team is available for an honest, no-pressure conversation about whether residential dual diagnosis treatment fits. There is no obligation in reaching out – only the chance to understand what help might actually look like.
A confidential conversation, whenever you are ready
The Holina team can speak with you or a family member about what a residential stay involves, who it suits, and what the first steps look like. No pressure, no obligation – just an honest conversation about whether this is the right fit.

About the Author
Yossi Zubari
CEO & Founder
Director and Senior Therapist working with addiction for over 25 years, and in personal recovery for almost 30 years.